EVO ICL™ – EVOlution in Visual Freedom
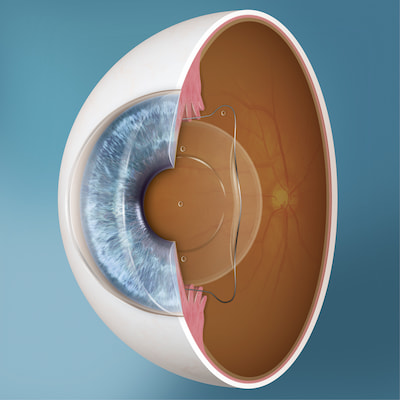
What is EVO ICL Lens?
EVO ICL is an Implantable Contact Lens (ICL) designed to correct nearsightedness with and without astigmatism. The small flexible lens is placed behind the iris (the colored part of the eye) and in front of the natural crystalline lens in order to improve vision. It’s like having your doctor implant a lens similar to a contact lens into your eye so you can live without the daily hassles and maintenance of typical contact lenses.
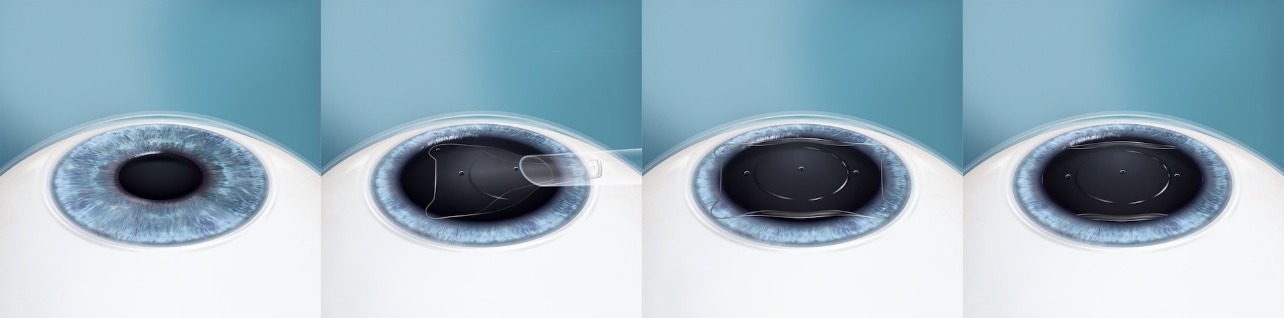
EVO ICL Procedure – What to Expect
EVO ICL lens is made of biocompatible Contact material that works in harmony with your eye. Your eye doctor will create a small opening in your cornea that will be used to insert and position the EVO ICL. For most patients, the procedure is virtually painless with numbing eye drops and it typically takes less than 20 – 30 minutes. Patients typically experience improved vision right away and a quick recovery time.
Benefits of EVO ICL
- Provides clear, sharp vision1,2
- 20 to 30-minute procedure
- Quick recovery time
- Removable by your doctor
- Offers UV protection
- Not visible once in place
- Can treat nearsightedness with or without astigmatism
- For patients who may not be candidates for LASIK or other vision correction procedures due to thin corneas3,4
- Does not cause dry eye syndrome5
- Excellent vision both day and night6,7
- Over 2 million ICLs distributed worldwide
- 99.4% of patients surveyed would have the EVO Lens procedure again8
Cost and Financing for EVO ICL
The cost of an EVO ICL procedure can vary depending on your personalized treatment plan. Many EVO ICL patients look forward to spending less in the long run with the EVO ICL compared to the continued costs of contacts and glasses. Ask about financing options and payment plans that may be available for your EVO ICL procedure.
Is EVO ICL Right for Me?
EVO ICL is well-suited for a wide variety of people. Ideal candidates for EVO ICL are aged 21 to 45 with nearsightedness, with or without astigmatism, and have maintained a stable prescription for at least one year. If you are seeking a solution to decrease or eliminate the cost and frustration of traditional contacts or glasses, EVO may be your answer. Contact us to discuss if EVO ICL is right for you.

“EVO has helped me to live life to the fullest with no more hesitation. I simply wake up and go about my day.”
– Joe Jonas
Book Your Consultation
If you would like to see if the EVO ICL is right for you, contact us today to schedule a consultation.

1 Sanders D, Vukich J. Comparison of implantable collamer lens (ICL) and laser-assisted in situ keratomileusis (LASIK) for Low Myopia. Cornea. 2006
2 Igarashi A, Kamiya K, Shimizu K, Komatsu M. Visual Performance after implantable Collamer lens implantation and wavefront-guided laser in situ keratomileusis for high myopia. Am J Opthalmol. 2009
3 Parkhurst G, Psolka M, Kezirian G. Phakic intraocular lens implantation in United States military warfighters: A retrospective analysis of early clinical outcomes of the Visian ICL. J Refract Surg. 2011;27(7):473-481
4 Gimbel H, et al. Management of myopic astigmatism with phakic intraocular lens implantation. Journal of Cataract & Refractive Surgery, Volume 28, Issue 5, 883 – 886.
5 Ganesh S, Brar S, Pawar A. Matched population comparison of visual outcomes and patient satisfaction between 3 modalities for the correction of low to moderate myopic astigmatism. Clin Ophthalmol. 2017 Jul 3;11:1253-1263.
6 Parkhurst GD. A prospective comparison of phakic collamer lenses and wavefront-optimized laser-assisted in situ keratomileusis for correction of myopia. Clin Ophthalmol. 2016 Jun 29;10:1209-15.
7 Ganesh S, Brar S, Pawar A. Matched population comparison of visual outcomes and patient satisfaction between 3 modalities for the correction of low to moderate myopic astigmatism. Clin Ophthalmol. 2017 Jul 3;11:1253-1263.
8 Packer M. The Implantable Collamer Lens with a central port: review of the literature. Clinical Ophthalmology 2018: 12: 2427–2438